


Overview
Transposition of the great arteries, also called TGA, is a serious, rare heart condition in which the two main arteries leaving the heart are switched. The condition is present at birth. That means it's a congenital heart defect.
Types
There are two types of transposition of the great arteries:
- Transposition of the great arteries, also called dextro-transposition of the great arteries (d-TGA). This type lowers the amount of oxygen-rich blood to the body. It's often diagnosed during pregnancy or soon after birth. Without treatment, serious complications or death can happen.
- Congenitally corrected transposition, also called levo-transposition of the great arteries (l-TGA or ccTGA). This is a less common type. Symptoms may not be seen right away. Treatment also depends on the specific heart structure and if there are other heart conditions.
Surgery to fix the positions of the arteries is the usual treatment. The surgery is usually done soon after birth.
Symptoms
Symptoms of transposition of the great arteries include:
- Blue or gray skin due to low oxygen levels. Depending on skin color, these color changes may be harder or easier to see.
- Pounding heartbeat.
- Weak pulse.
- Lack of appetite.
- Poor weight gain.
Some people with the congenitally corrected type of TGA may not have symptoms for many years.
Also, skin color changes may not be seen right away if a baby with TGA also has other heart changes that let some oxygen-rich blood move through the body. But as the baby becomes more active, less oxygen-rich blood flows through the body. The changes in skin color become more noticeable as oxygen levels drop.
When to see a doctor
Serious congenital heart defects are often diagnosed before or soon after a child is born.
Get help right away if a child has trouble breathing.
Also get emergency medical help for anyone who has blue or gray skin or nails. Low oxygen levels can cause this change in skin color. Depending on skin color, the changes may be harder or easier to see.
Causes
Transposition of the great arteries, also called TGA, happens during pregnancy when the unborn baby's heart is forming. An unborn baby also is called a fetus. The cause is most often not known.
To understand TGA, it may help to know how the heart usually pumps blood. The typical heart has four chambers.
- The two upper chambers are called the atria.
- The two lower chambers are called the ventricles.
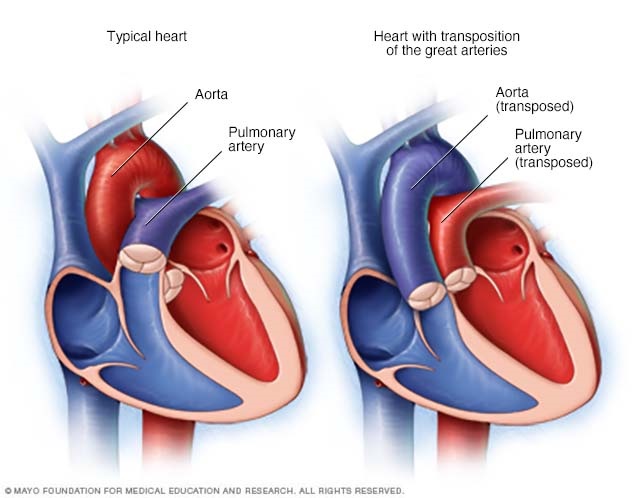
The artery that carries blood from the heart to the lungs is called the pulmonary artery. It connects to the heart's lower right chamber, called the right ventricle.
The right side of the heart moves blood to the lungs. In the lungs, blood picks up oxygen and then returns it to the heart's left side. The left side of the heart then pumps the blood through the body's main artery, called the aorta. The blood then goes out to the rest of the body.
Transposition of the great arteries, also called d-TGA
In this condition, also called dextro-transposition of the great arteries (d-TGA), the position of the two arteries leaving the heart is switched. The pulmonary artery connects to the left lower heart chamber. The aorta connects to the right lower heart chamber.
The switched arteries cause changes in blood flow. Usually, oxygen-poor blood flows through the right side of the heart to the lungs to get oxygen. In d-TGA, the oxygen-poor blood goes from the right side of the heart to the aorta and the rest of the body. The oxygen-rich blood goes back into the lungs without being pumped to the rest of the body. Unless there also is a hole in the heart, such as an atrial septal defect, that lets the blood mix, the body does not get oxygen-rich blood. This is life-threatening.
Congenitally corrected transposition, also called ccTGA or l-TGA
In this less common type, also called levo-transposition of the great arteries, the two lower heart chambers are reversed.
- The lower left heart chamber, called the left ventricle, is on the heart's right side. It gets blood from the upper right heart chamber.
- The lower right heart chamber is on the heart's left side. It gets blood from the left upper heart chamber.
The blood usually still flows the right way through the heart and body. But the heart can have long-term trouble pumping blood. People with l-TGA also may have changes with the tricuspid heart valve such that it does not work as well.
Risk factors
Possible risk factors for congenital heart defects such as transposition of the great arteries include:
- Rubella, also called German measles. Having rubella during pregnancy can cause changes in an unborn baby's heart development. A blood test done before pregnancy can determine if you're immune to rubella. A vaccine is available if you aren't.
- Some medicines. Taking certain medicines during pregnancy can cause congenital heart defects and other health conditions present at birth. Always tell your healthcare team about the medicines you take.
- Alcohol use. Drinking alcohol during pregnancy raises the risk of congenital heart defects in the baby.
- Smoking. If you smoke, quit. Smoking during pregnancy can be harmful to the unborn baby, also called a fetus.
- Diabetes. Careful control of blood sugar before and during pregnancy can reduce the risk of congenital heart defects in the baby. Diabetes that develops during pregnancy is called gestational diabetes.
Complications
Complications depend on the type of transposition of the great arteries. Possible complications of complete transposition of the great arteries may include:
- Not enough oxygen to body tissues. Unless there's some mixing of oxygen-rich blood and oxygen-poor blood within the heart, this complication causes death.
Possible complications of congenitally corrected transposition, also called l-TGA, may include:
- Complete heart block. Transposition of the great arteries can change the way electrical signals move through the heart and tell the heart to beat. A complete heart block occurs if all signals are blocked.
- Heart valve disease. In l-TGA, the valve between the upper and lower heart chambers, called the tricuspid valve, may not close all the way. Blood might flow backward. This condition is called tricuspid valve regurgitation. It can make it harder for the heart to pump blood.
- Heart failure. The heart can't pump enough blood to meet the body's needs. Heart failure may happen over time in l-TGA because the right lower heart chamber is pumping under higher pressure than usual. The strain may make the muscle of the right lower chamber weak.
Pregnancy and TGA
If you had transposition of the great arteries and want to become pregnant, talk with your healthcare professional. It may be possible to have a healthy pregnancy. But special care may be needed.
Complications of TGA, such as changes in heart signaling, may make pregnancy risky. Pregnancy isn't recommended for people who have severe complications of TGA, even if they had surgery to fix the heart condition.
Prevention
Because the exact cause of most congenital heart defects is not known, it may not be possible to prevent these conditions.
If you have a family history of heart conditions present at birth, talk with a genetic counselor and a healthcare professional trained in congenital heart defects before getting pregnant.
It's important to take steps to have a healthy pregnancy. Get proper prenatal care. Before becoming pregnant, get recommended immunizations. Start taking a multivitamin with folic acid. Folic acid has been shown to prevent harmful changes in the unborn baby's brain and spinal cord. It also may help reduce the risk of congenital heart defects.
Diagnosis
Transposition of the great arteries, also called TGA, is often diagnosed before birth during a routine pregnancy ultrasound. If not, it is diagnosed soon after birth.
Immediately after birth, a healthcare professional listens to the baby's heart and lungs. A whooshing heart sound, called a murmur, may be heard while listening to the baby's heart. Some murmurs are caused by blood flow changes to and from the heart.
Tests
Tests to diagnose transposition of the great arteries include:
- Echocardiogram. Sound waves make images of the beating heart. An echocardiogram shows how blood moves through the heart and heart valves. It can tell if the two main arteries leaving the heart are in the correct position. If the test is done on an unborn baby before birth, it's called a fetal echocardiogram.
- Chest X-ray. This test shows the condition of the heart and lungs. It can't diagnose TGA by itself, but it helps show the heart's size.
- Electrocardiogram (ECG or EKG). This simple test shows how the heart is beating. Sticky patches with sensors on them go on the chest and sometimes the arms and legs. Wires connect the sensors to a computer, which prints or displays the test results.
- Pulse oximetry. A sensor placed on the fingertip records the amount of oxygen in the blood. Too little oxygen may be a sign of a heart or lung condition.
Treatment
Treatment depends on the type of transposition of the great arteries.
All babies with complete transposition of the great arteries, also called d-TGA, need surgery soon after birth to fix the heart.
Treatment for congenitally corrected transposition, also called l-TGA, depends on:
- When the condition is diagnosed.
- What other heart conditions exist.
Medications
Before heart repair surgery, the baby may get a medicine called prostaglandin (Prostin Vr Pediatric) . The medicine increases blood flow. It helps oxygen-poor and oxygen-rich blood better mix together.
After surgery to fix TGA, medicines are given to help the heart work better. Medicines may be needed to:
- Control the heartbeat.
- Manage blood pressure.
- Help the body remove fluid.
Surgery or other procedures
Surgery for transposition of the great arteries, also called TGA, is usually done within the first days to weeks after birth. The specific surgery done depends on the type of TGA. Some people with congenitally corrected transposition do not need surgery.
Treatment may include:
- Atrial septostomy. This treatment may be done right away as a temporary fix before surgery. It uses thin tubes and small cuts to widen a natural connection between the heart's upper chambers. Doing this helps mix oxygen-rich and oxygen-poor blood, improving oxygen levels in the baby's body.
- Arterial switch operation. This is the most common surgery used to correct transposition of the great arteries. A surgeon moves the two main arteries, leaving the heart to their correct positions. The surgeon also has to move the coronary arteries. Other heart conditions present at birth may be repaired during this surgery.
- Atrial switch operation. The surgeon splits blood flow between the heart's two upper chambers. After this surgery, the right lower heart chamber must pump blood to the body, instead of just to the lungs.
- Rastelli operation. This surgery may be done if a baby with TGA also has a hole in the heart called a ventricular septal defect. The surgeon patches the hole and redirects blood flow from the left lower heart chamber to the aorta. This lets oxygen-rich blood go to the body. An artificial valve connects the right lower heart chamber to the lung artery.
- Double switch procedure. This complex surgery is used to treat congenitally corrected transposition. It switches the great artery connections so the left lower heart chamber can pump oxygen-rich blood to the aorta.
Babies born with TGA often have other heart conditions. Other heart surgeries may be needed. Surgery also may be needed to treat complications of TGA. If TGA causes changes in the heartbeat, a device called a pacemaker may be needed.
After surgery to fix TGA, regular health checkups are needed for life. A doctor trained in heart conditions present at birth usually cares for a baby with transposition of the great arteries. This type of doctor is called a congenital cardiologist.
Every situation is different. But due to advances in surgery, most babies with transposition of the great arteries grow up to lead active lives.
Coping and support
Caring for a baby with a serious heart condition, such as transposition of the great arteries, can be challenging. These tips might help.
- Get support. Ask for help from family members and friends. Talk with your baby's healthcare team about support groups and other types of assistance that are available near you.
- Keep notes about the baby's health history. Write down the diagnosis, medicines, surgeries and other treatments. Include the dates of treatments and the names and phone numbers of all the healthcare professionals. Such notes are helpful for healthcare professionals who are unfamiliar with your baby's health history.
- Ask about activities and sports. After surgery to fix TGA, some high-energy activities might not be safe to do. Talk with a healthcare professional about which exercises or activities are safe.
Preparing for an appointment
A life-threatening congenital heart defect is usually diagnosed soon after birth. There may not be time to prepare for the appointment.
If you think your baby has symptoms of a heart condition, talk with a healthcare professional. You may be sent to a doctor trained in heart conditions present at birth, called a congenital cardiologist.
Here's some information to help you prepare for any appointments.
What you can do
Take someone with you to the appointment, if possible. Sometimes it can be hard to remember all of the information that you get. Someone who goes with you may be able to remember details.
Make a list of:
- Your child's symptoms, if any. Include those that may seem unrelated to transposition of the great arteries. Also note when they started.
- Important personal information, including a family history of congenital heart defects. Ask if anyone in your family was born with a heart condition.
- Questions to ask the healthcare professional.
For transposition of the great arteries, some questions to ask the healthcare professional are:
- Does my baby need surgery?
- What other treatments are available? Which do you recommend?
- How often does my baby need health checkups?
- Are there any activity limits?
- Is there any information that I can take home with me? What websites do you recommend?
Don't hesitate to ask other questions.
What to expect from your doctor
Your healthcare team usually asks you many questions, such as:
- Was anyone in your family born with a heart condition?
- Were there any pregnancy complications?
- Has your child been growing and meeting developmental milestones as expected? Ask your child's pediatrician if you're not sure.
© 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use