


Overview
Pediatric obstructive sleep apnea is a condition in which a child's breathing is partly or completely blocked during sleep. Breathing can briefly stop and start again many times a night. The condition happens when the upper airway narrows or is blocked during sleep.
Obstructive sleep apnea can look different in children than it does in adults. Adults usually have daytime sleepiness. Children are more likely to have behavior issues, such as acting hyper or not paying attention. Risk factors also differ. In adults, the key risk factors are obesity and age. Although obesity can play a role in children, the main risk factor in children is having tonsils and adenoids that are larger than usual. The adenoids are two small pads of tissue in the back of the nose. The tonsils are two oval-shaped pads in the back of the mouth.
It's important for healthcare professionals to find and treat pediatric obstructive sleep apnea as soon as possible. Early treatment helps prevent other health conditions called complications. These can affect children's growth, learning, behavior and heart health. The first treatment may be surgery to remove enlarged tonsils and adenoids. But some children may get better using medical devices or taking medicines.
Symptoms
During sleep, symptoms of pediatric obstructive sleep apnea can include:
- Snoring.
- Pauses in breathing.
- Restless sleep.
- Snorting, gasping, coughing or choking.
- Mouth breathing.
- Nighttime sweating.
- Bed-wetting that starts after a long period of dry overnights.
Infants and young children with obstructive sleep apnea don't always snore. They might just have disturbed sleep.
During the day, children with sleep apnea might:
- Get headaches in the morning.
- Breathe through the mouth or have trouble breathing through the nose.
- Have trouble learning and paying attention.
- Do poorly in school.
- Have behavior issues such as acting hyper, impulsive or aggressive.
- Have poor weight gain.
- Talk about feeling sleepy, or fall asleep during school or during short car or bus rides.
When to see a doctor
See your child's healthcare professional if your child has any symptoms of obstructive sleep apnea, including frequent snoring.
Causes
Pediatric obstructive sleep apnea is caused by muscles in the back of the throat relaxing and blocking the upper airway. In children, this leads to pauses in breathing that last about twice as long as the typical breath.
When breathing stops, this triggers the brain to wake up so that the airway can open again. This makes it hard to get enough rest.
Various conditions can raise the risk of the upper airway becoming blocked during sleep. Commonly, enlarged tonsils in the back of the mouth and enlarged adenoids in the back of the nose can cause a blockage. Other possible causes include being born with a birth defect related to the shape of the face or head and certain health conditions.
Risk factors
The main risk factor for pediatric obstructive sleep apnea is enlarged tonsils and adenoids, especially in younger children. Obesity also is an important a risk factor, mainly among teenagers.
Other risk factors for pediatric sleep apnea include having:
- A genetic condition such as Down syndrome or Prader-Willi syndrome.
- Birth defects in the skull or face.
- A group of conditions called cerebral palsy that affect movement and posture.
- A group of inherited blood disorders known as sickle cell disease.
- Conditions called neuromuscular disorders that affect the function of muscles due to problems with the nerves and muscles in the body.
- A history of low birth weight.
- A family history of obstructive sleep apnea.
Complications
Without treatment, pediatric obstructive sleep apnea can lead to other health conditions called complications. Rarely, pediatric obstructive sleep apnea can cause infants and young children not to grow as much as those who don't have the condition. Children who don't receive treatment also may have a higher risk of later complications such as:
- High blood pressure.
- High cholesterol.
- A higher than typical blood sugar level that raises the risk of diabetes.
- Other heart and blood vessel conditions.
Very rarely, children with certain genetic conditions can have serious symptoms of pediatric obstructive sleep apnea. These symptoms can lead to death. But in most children, treatment can help manage complications.
Diagnosis
Diagnosis involves the steps that a healthcare professional takes to find out if your child has pediatric obstructive sleep apnea. A healthcare professional reviews your child's symptoms and health history and does a physical exam. Your child's healthcare professional likely will look at your child's head, neck, nose, mouth and tongue.
Other tests might be needed as well. The main test to check for sleep apnea in children is called a polysomnogram. This involves an overnight sleep test. Sensors are placed on your child's body. The sensors record brain waves, breathing patterns, snoring, oxygen levels, heart rate and muscle activity while your child sleeps. This test may take place at a sleep center.
Treatment
Your child's healthcare professional works with you to find the right treatment for your child's pediatric obstructive sleep apnea. Most often, the first treatment for the condition is surgery to remove enlarged tonsils and adenoids. This is called adenotonsillectomy (ad-uh-no-ton-sil-EK-tuh-me). But some children get better with medicines or medical devices.
The right treatment plan for your child depends on your child's sleep apnea symptoms and risk factors. For most children, treatment includes adenotonsillectomy, but your child's healthcare professional may recommend other treatments if this surgery isn't right for your child. Other treatments also may be needed if the surgery doesn't fully treat your child's obstructive sleep apnea.
Some kids get better without sleep apnea treatments. It's possible for some children with mild to moderate obstructive sleep apnea to outgrow the condition. A healthcare professional may recommend closely watching a child for up to six months to see if the symptoms get better. This is called watchful waiting. If the child also has allergies or other conditions that irritate the airway, watchful waiting can include treatment for those.
Medications
Topical nasal steroids might ease sleep apnea symptoms for some children with mild obstructive sleep apnea. These medicines include fluticasone (Flovent HFA, Xhance, others) and budesonide (Rhinocort, Pulmicort Flexhaler, others). For kids with allergies, montelukast (Singulair) might help relieve symptoms when used alone or with nasal steroids.
Therapies
Your child's healthcare professional may recommend use of devices such as:
-
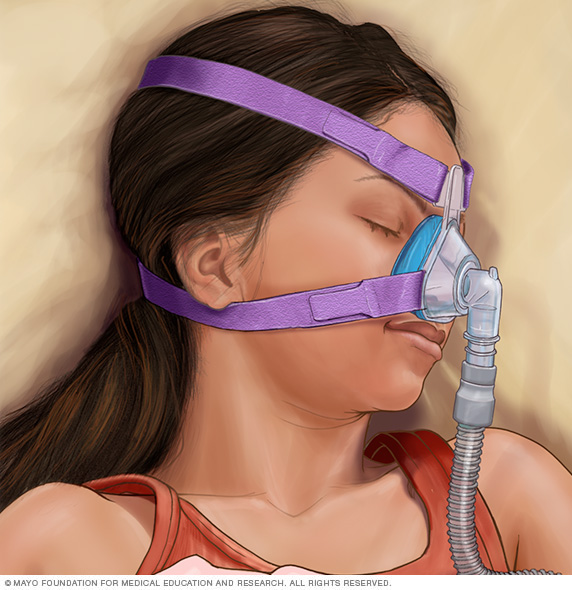
Positive airway pressure therapy. Small machines gently blow air through a tube with treatments called continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BPAP). The tube is attached to a mask that goes around your child's nose or nose and mouth during sleep. The machine sends air pressure into the back of your child's throat to keep your child's airway open. Often, positive airway pressure therapy is a treatment option if medicines or removal of adenoids and tonsils doesn't work.
Proper fitting of the mask and refitting as your child grows can make the mask more comfortable to wear.
- Oral appliances. These devices go in the mouth. They include dental devices and mouthpieces. Oral appliances help to expand the roof of the mouth and nasal passages. They also might move your child's bottom jaw and tongue forward to keep the upper airway open. Only some children benefit from these devices.
Surgery or other procedures
Adenotonsillectomy to remove the tonsils and adenoids might improve obstructive sleep apnea by opening the airway. It's often a treatment option for children with moderate to severe obstructive sleep apnea. Your child's primary healthcare professional might refer you to a pediatric ear, nose and throat specialist to talk about surgery. Other forms of upper airway surgery might be recommended based on your child's condition.
Lifestyle and home remedies
You can take the following steps at home to help your child with pediatric obstructive sleep apnea:
- Stay away from airway irritants and allergens. Allergens are things that cause allergies. Keep your child away from tobacco smoke and other indoor allergens or pollutants. This step is important for all children, but especially those with obstructive sleep apnea. Irritants and allergens can irritate the airway and cause congestion.
- Weight loss. If your child is obese, ask your child's healthcare professional about a weight-loss plan. The healthcare professional can give you and your child information on healthy changes in diet and physical activity. You also may be referred to specialists in managing obesity because it is a complex disease. Weight-loss surgery is a treatment option for some teenagers who have obstructive sleep apnea and severe obesity.
- Watchful waiting. Some children may outgrow their obstructive sleep apnea while their healthcare professionals track their health. This is especially true for kids with mild disease and no other risk factors.
Preparing for an appointment
You'll likely start by seeing your child's regular healthcare professional. Or you might be referred right away to an ear, nose and throat specialist or a sleep medicine specialist.
Here's some information to help you get ready for your appointment.
What you can do
Make a list of:
- Your child's symptoms, including any that don't seem related to the reason for your appointment.
- All medicines, vitamins or other supplements your child takes, including the doses.
- Questions to ask your healthcare professional.
For pediatric obstructive sleep apnea, some basic questions to ask your child's healthcare professional include:
- What tests are needed?
- Is this condition likely short term or long term?
- What's the best course of action?
- Aside from the main treatment you're suggesting, are there other treatment options?
- Should I take my child to a specialist?
- Are there brochures or other printed material I can have? What websites do you recommend?
Feel free to ask other questions.
What to expect from your doctor
Your child's healthcare professional is likely to ask you questions such as:
- Does your child snore?
- What else have you noticed about your child's sleep?
- Does your child have trouble paying attention?
- Does your child have trouble with learning?
- Do you have a family history of obstructive sleep apnea?
© 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use